ICM+ software empowers clinical research into finding metrics derived from continuous high resolution monitoring data that are linked to insults such as disturbed intracranial dynamics, cerebral hypoperfusion and loss of cerebral autoregulation.
Transient and sustained increases in intracranial pressure (ICP)
Elevated intracranial pressure can occur in the form of short-lived ‘plateau waves’ or refractory intracranial hypertension. Plateau waves are thought to occur due to a cerebral vasodilatory cascade where increased cerebral blood within the skull causes marked increases of intracranial pressure and decreases of cerebral perfusion pressure. The decrease in cerebral perfusion pressure causes further dilation (an auto regulatory response) and aggravates the increased intracranial pressure (Rosner and Beck, 1984). At the peak of the plateau, the brain is hypo-perfused and hypoxia. Hypoperfusion can be monitored on ICM+ with thermodilution probes, transcranial Doppler ultrasound while cerebral hypoxia can be monitored with near infrared spectroscopy (NIRS) or brain tissue oxygenation (Dias et al., 2015, Lang et al., 2014).
Refractory intracranial hypertension also results in decreases in brain oxygenation and disturbed pressure reactivity (Czosnyka et al., 2016, Balestreri et al., 2004). Since severe refractory intracranial hypertension carries a high mortality, identifying early indicators that might predict raised ICP is an active area of research. Disturbed cerebral autoregulation may denote a higher risk of subsequent raised ICP (Czosnyka et al., 2016, Guiza et al., 2013).
Increased ICP is related to unfavourable patient outcome 6-months after the injury (Cabella et al., 2016).
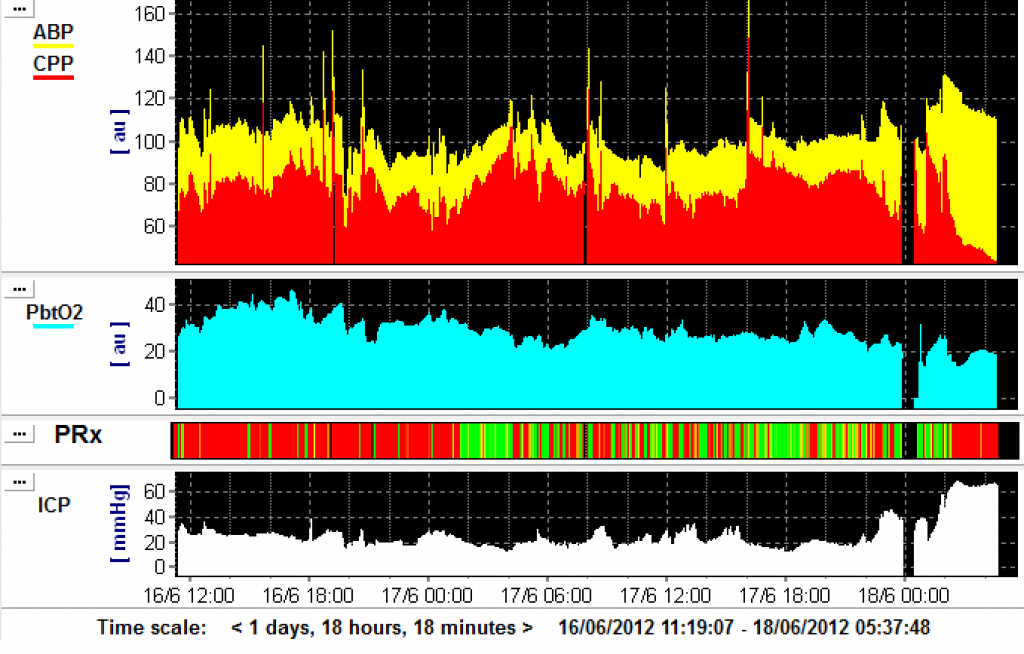
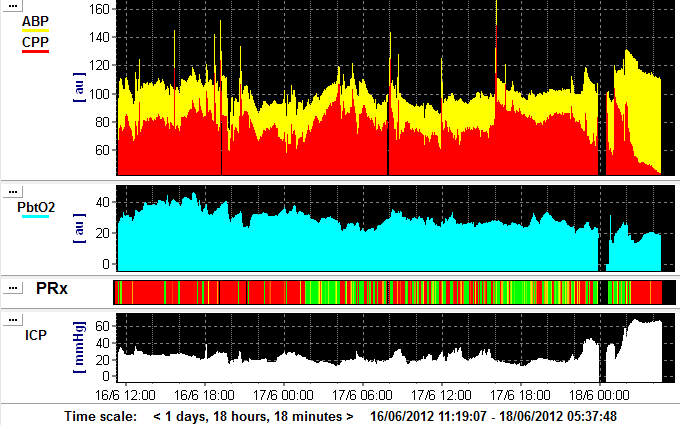
This patient develops refractory intracranial hypertension after almost a day of fluctuating ICP between 20 and 30 mm Hg. During the final rise in ICP, brain tissue oxygenation decreases to less than 20 mm Hg and PRx becomes disturbed (red line on risk chart). View image
{kind=link}
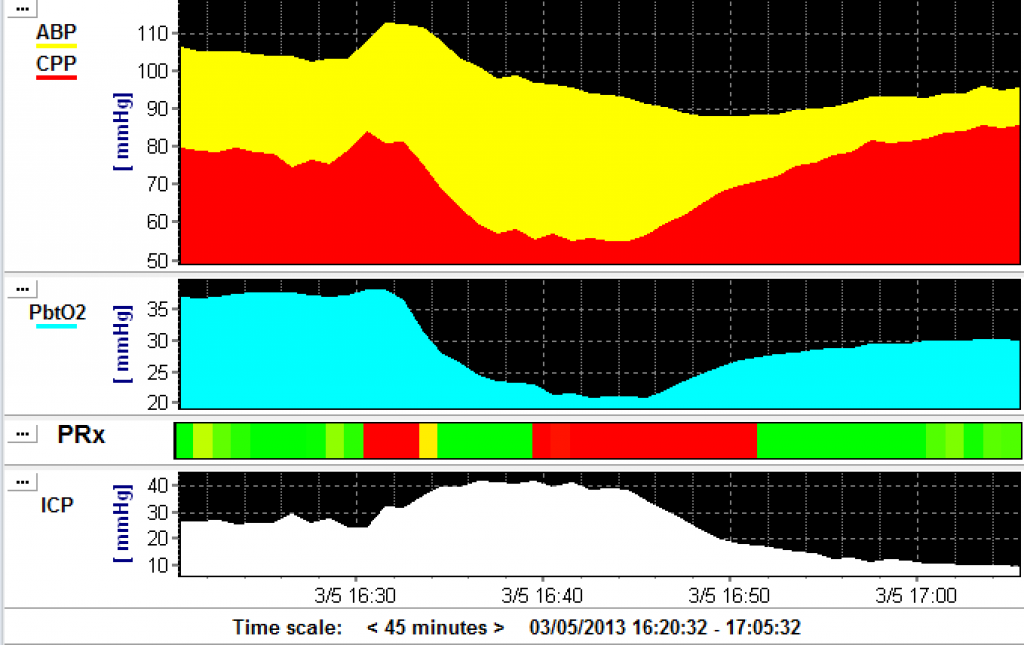
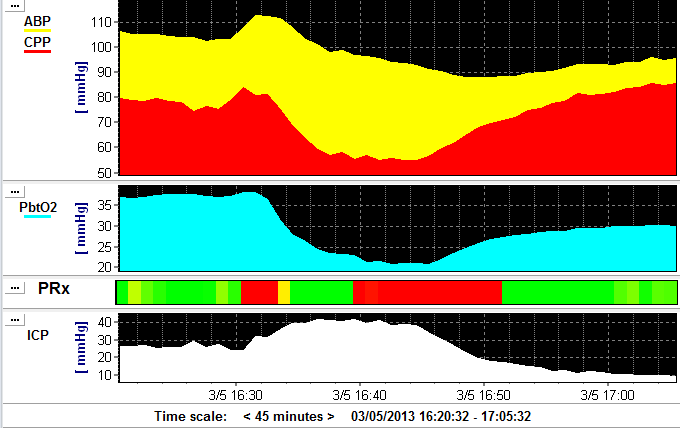
During this plateau wave, ICP rises to around 40 mm Hg and is associated with a decrease in CPP, brain oxygenation (PbtO2), and a disturbance of PRx as indicated by the red of the risk chart (3rd panel). View image
{kind=link}