ICM+ can be used to record and subsequently analyse high resolution data retrieved from bed-side monitors using a variety of digital and analogue interfaces. Signals such as cerebral blood flow (Hemedex), brain tissue oxygenation and temperature (Licox), near infrared spectroscopy, end-tidal CO2, etc., can be integrated with arterial and intracranial pressures.
These cases highlight the influence of carbon dioxide on intracranial variables such as brain oxygenation, intracranial pressure, and pressure reactivity. Although hyperventilation is often used to control intracranial pressure, the decrease in carbon dioxide can also lead to a decrease in PBTO2. Combining PBTO2 data with arterial blood pressure and intracranial pressure can give an indication of episodes of cerebral hyperaemia.
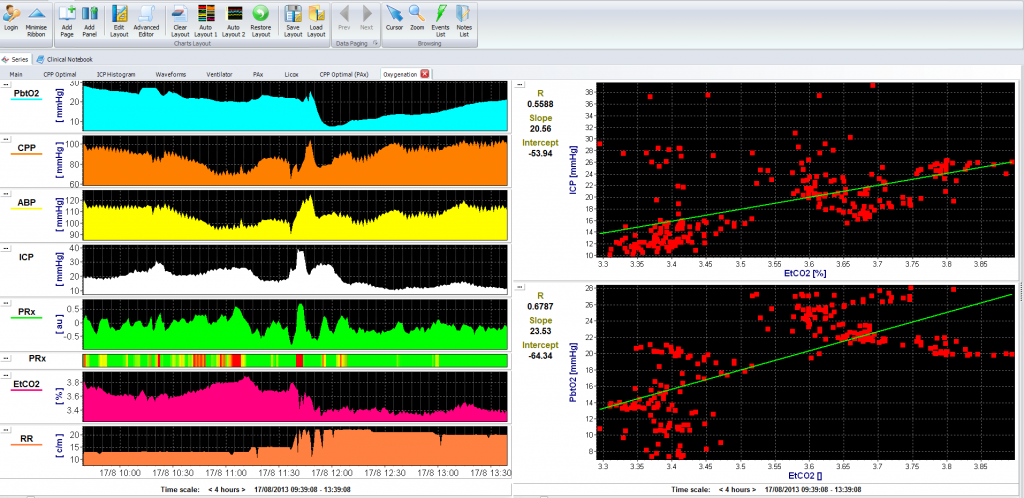
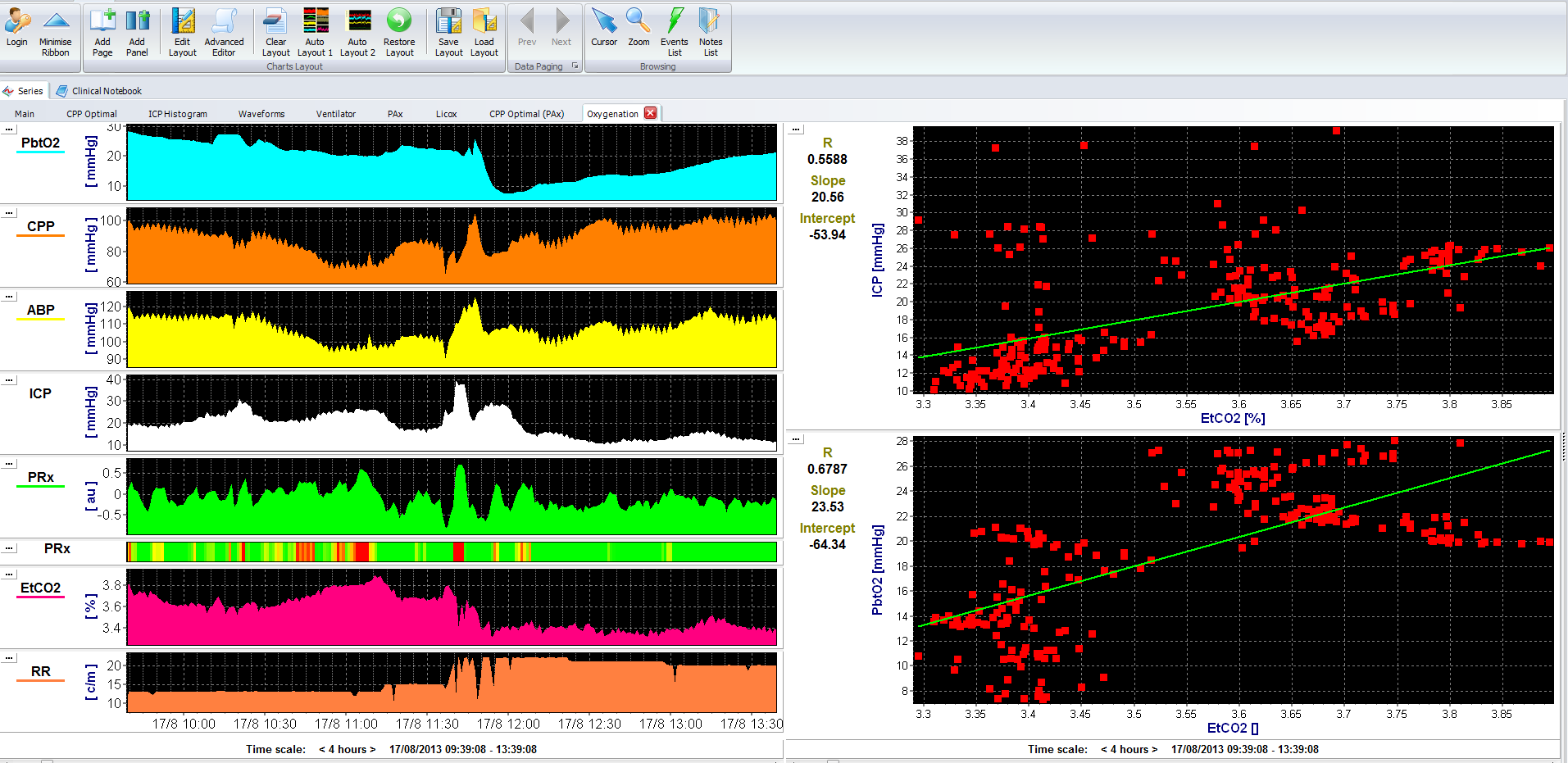
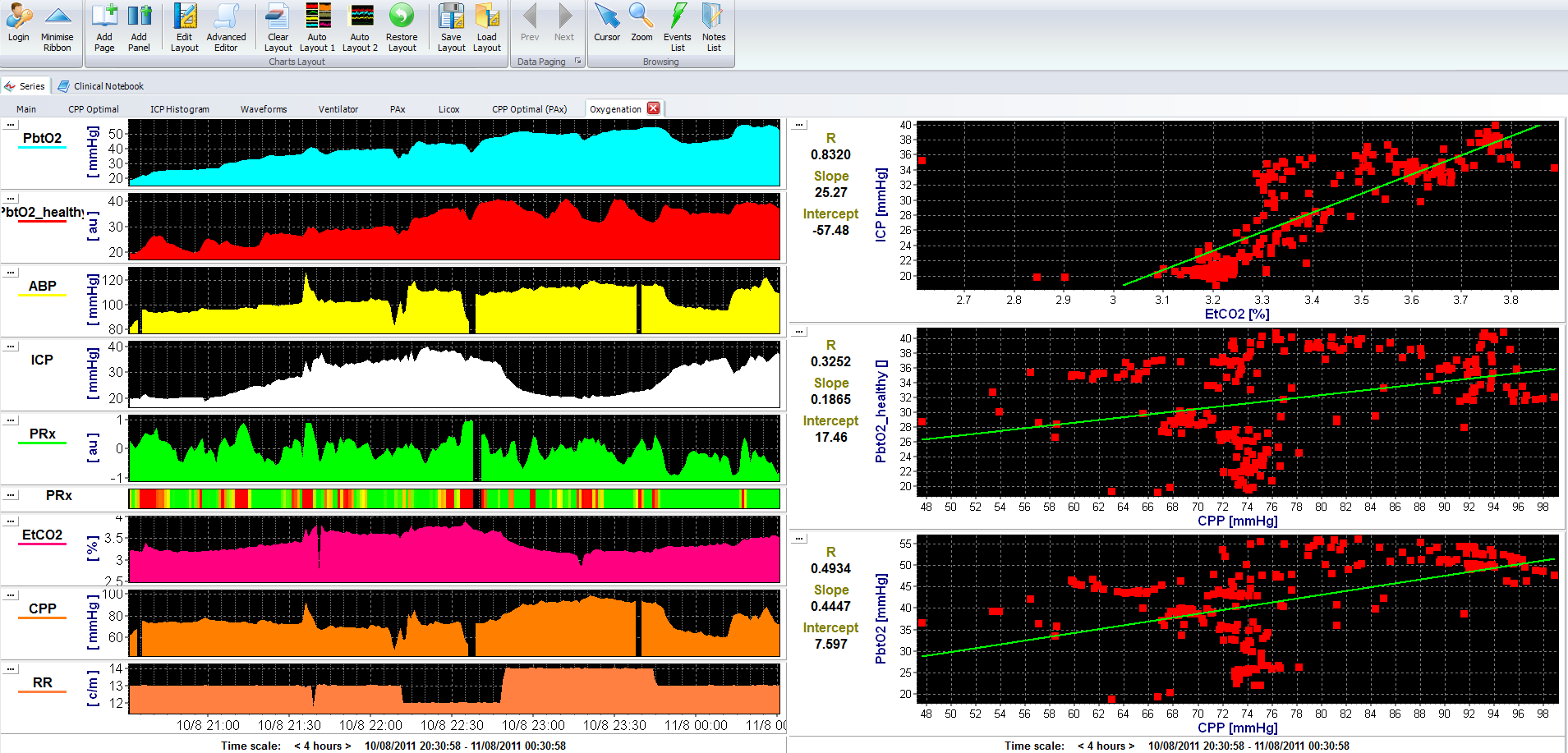
Just after 11:30, ICP increases to 40 mm Hg. Ventilation is increased at this time, as noted by the increase in respiratory rate (RR-bottom) from 15 to 20 breaths per minute, and the decrease in PetCO2 from 3.7 kPa to 3.4 kPa. This decrease in etCO2 resulted in a decrease in brain tissue oxygenation (top, from 20 to 10 mm Hg) and ICP (from 40 to 30 mm Hg), probably both as a result of cerebral vasoconstriction. For each 1kPa decrease in etCO2, ICP decreases by ~21 mm Hg and PbTO2 decreases by 24 mm Hg (right panel). View image
{kind=link}
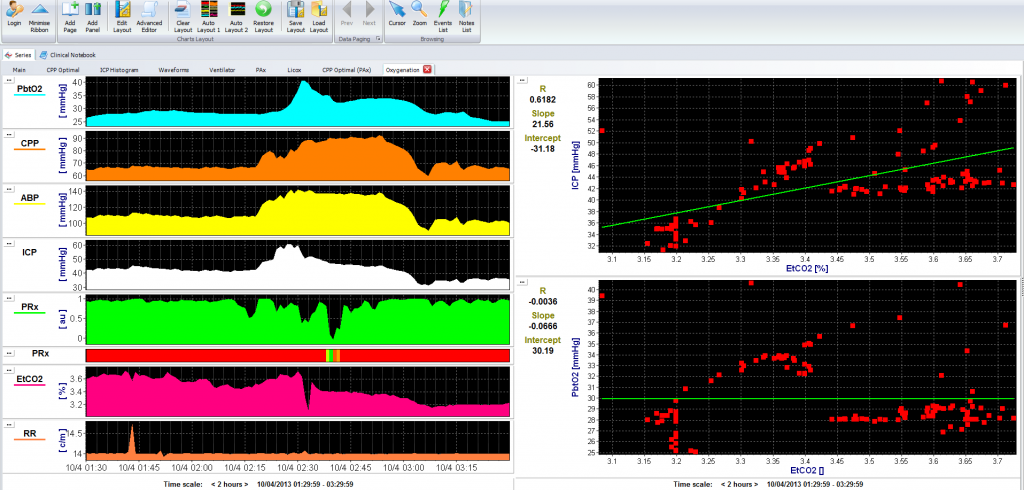
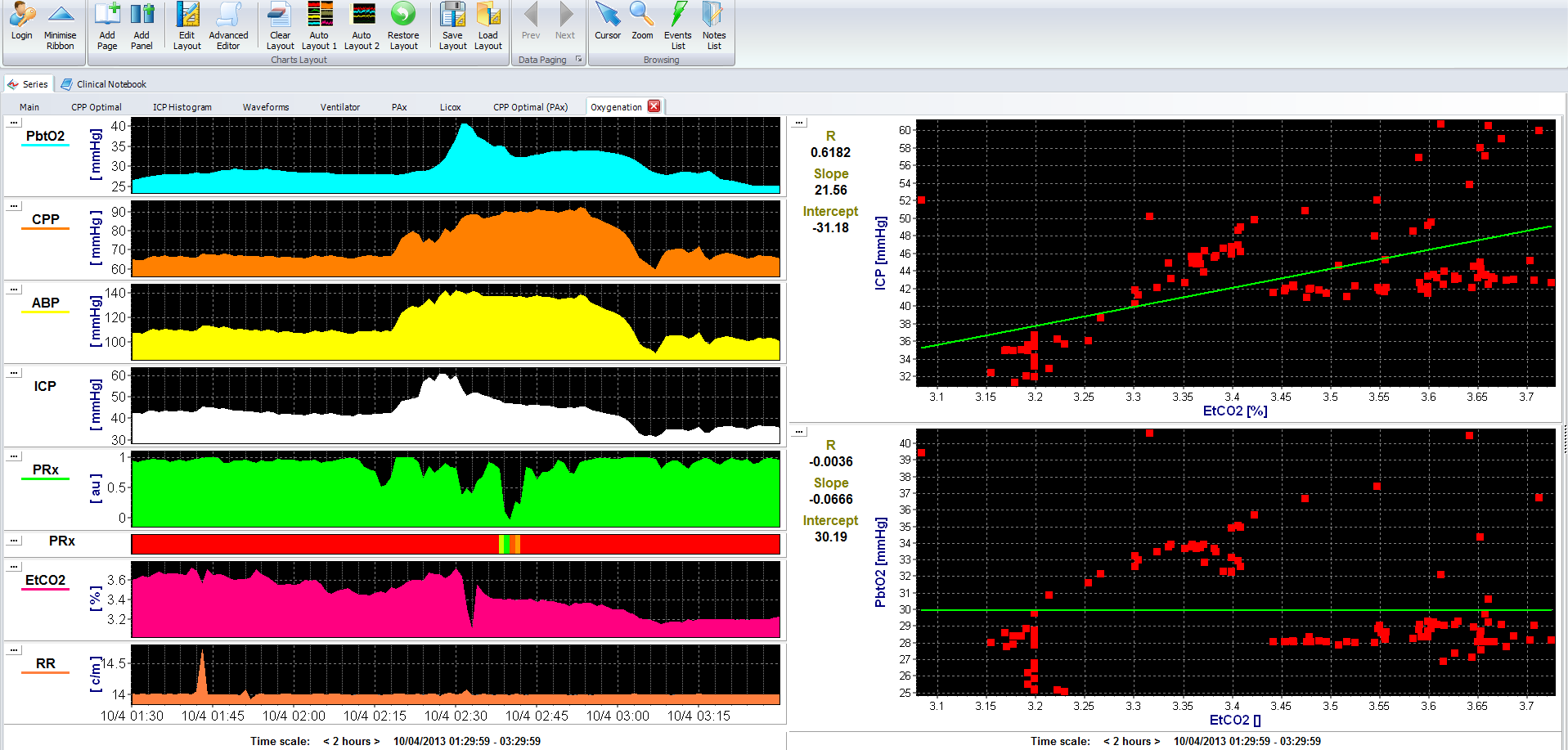
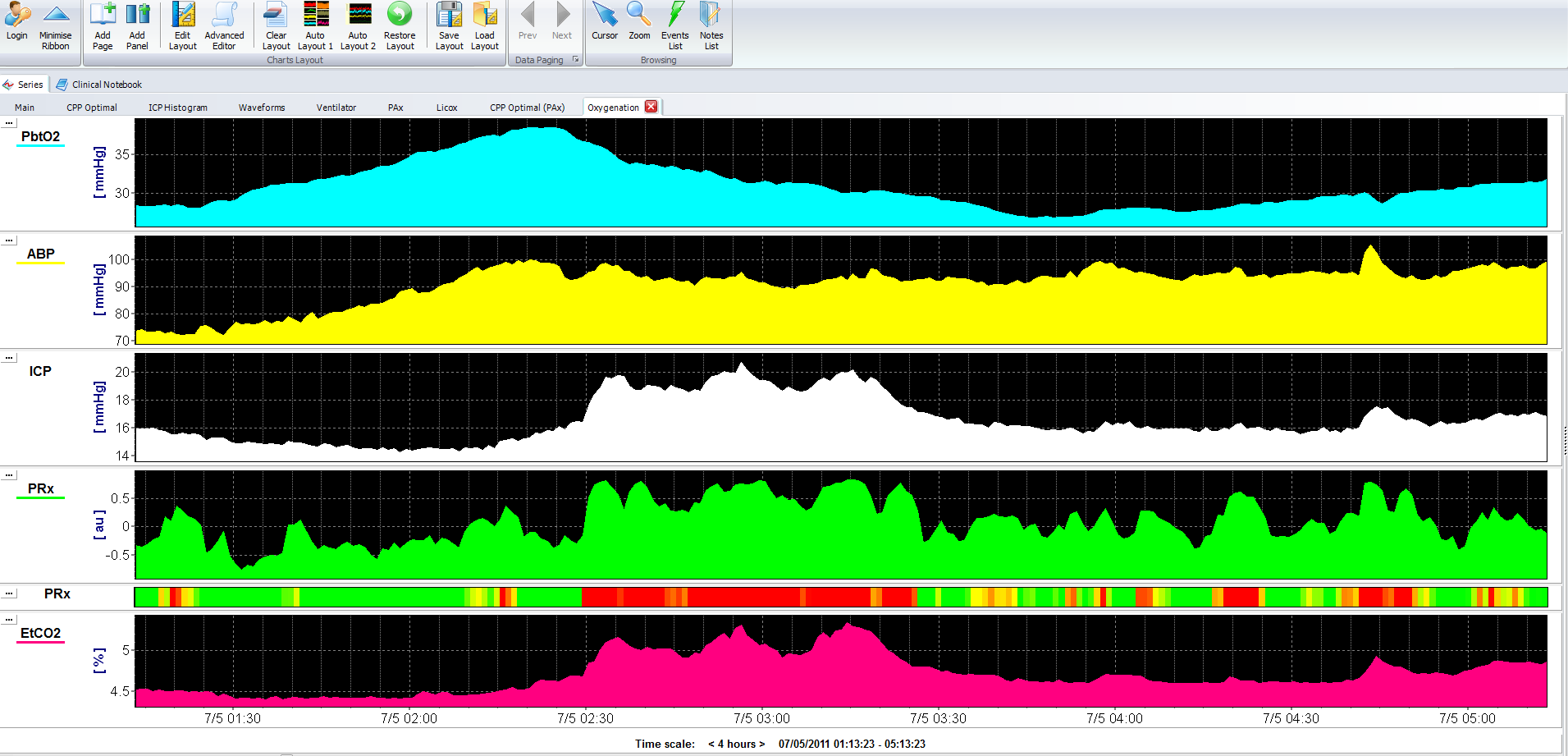
At 02:15, ABP increases from 100 to 140 mm Hg, resulting in an increase in CPP from 65 to 90 mm Hg. Probably as a consequence, the grossly-disturbed pressure reactivity (PRx ~ +1, solid red line), and increase in ABP causes an increase in brain tissue oxygenation and ICP. View image
{kind=link}
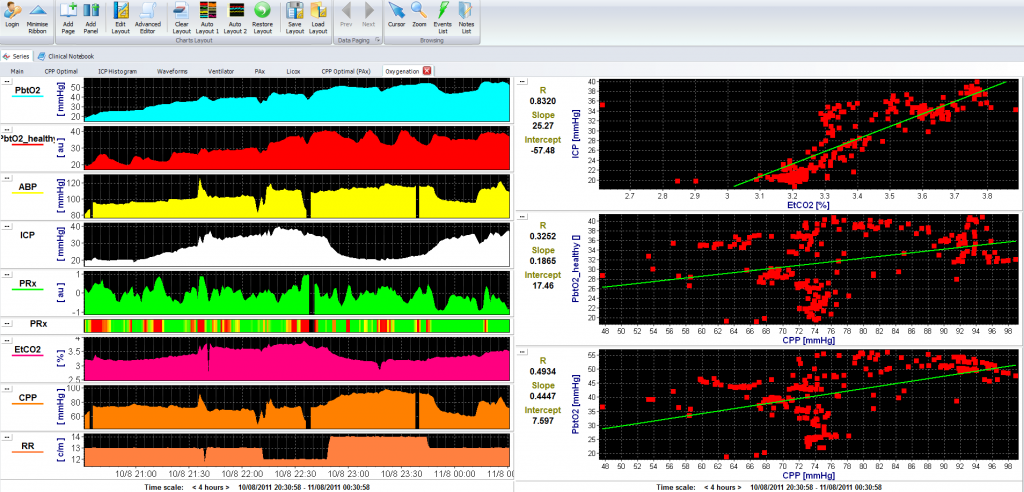
In this case changes in ICP follow changes in etCO2 (Pearson correlation 0.83). Oxygenation is measured in the pericontusional tissue (top panel, light blue) and contralateral ‘healthy tissue’ (red). View image
{kind=link}
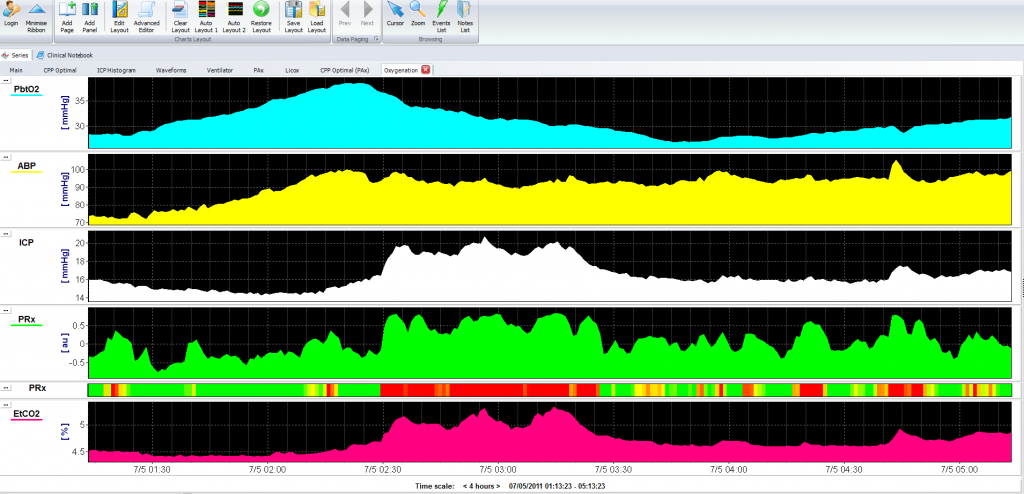
In this case, etCO2 increases from 4.5 to 5.2 kPa. Associated with this is an increase in ICP from 16 to 20 mm Hg and a disturbance of pressure reactivity (PRx >0.5, solid red line). Brain oxygenation, however, in this case seems to follow changes in ABP (top two panels). View image
{kind=link}